
It’s time to
 push the limits
push the limits
of what BCL-2 inhibition can achieve
Across hematologic malignancies,
Advancing BCL-2 inhibition means redefining
what should be expected:

Broad applicability across diseases

Suitability for
a wide range
of patients

Minimal impact on patients’ lives

Optimal disease control


Expanding the use of BCL-2 inhibition
The potential of synergistic combinations has yet to be fully realized across hematologic malignancies1

Evidence that reflects reality
Pushing the limits of BCL-2 inhibition demands clinical evidence in populations that are reflective of the patients and diverse disease types encountered in everyday practice1,7
BCL-2 inhibition must be rigorously assessed across the full:
Spectrum of patient characteristics8

- From treatment-naïve to heavily pretreated
- Age
- Comorbidities
- Fitness
Continuum of disease1,7

- From indolent to high-risk and mutated disease
- In relapsed and resistance settings (eg, G101V)

Limited disruption to daily living
Leveraging the full potential of BCL-2 inhibition requires addressing practical burdens9
Reduced time spent in the clinic
Less frequent office visits
Fewer required hospitalizations
- Simplified monitoring, while maintaining patient safety, should serve as a guiding ambition, ensuring that treatment is both practical and patient-centered10

Undetectable MRD (uMRD) is emerging as a new benchmark that reflects rapid, deep, and sustained disease control in hematologic malignancies11,12*
MRD positivity is associated with worse outcomes7,13-15
Current regimens may underperform in delivering deep MRD responses, leaving residual disease that can drive relapse and earlier progression
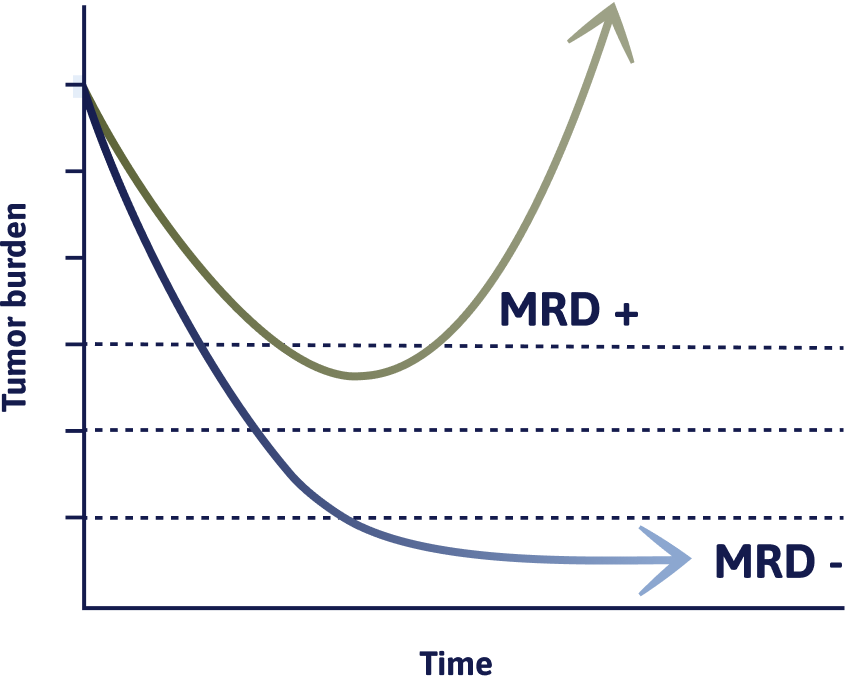

Achieving uMRD is associated with
vs detectable MRD
Reliability of response matters16,17
In clinical trials, BCL-2 inhibition should demonstrate consistent uMRD rates across†:

Peripheral bloodBone marrow
*Currently, uMRD is not an accepted endpoint for regulatory drug approval in B-cell malignancies.
†In BCL-2 inhibitor–treated AML and MM, MRD negativity has only been assessed in bone marrow. Data demonstrating concordant MRD assessments in peripheral blood and bone marrow in these malignancies are lacking. 14,15,18-20

Follow our progress as we continue to push the limits of BCL-2 inhibition
Sign up to receive updates on advancements in BCL-2 inhibition and hematologic malignancy research.
By submitting your email, you agree to receive educational updates. You may unsubscribe at any time.
AML=acute myeloid leukemia; BCL-2=B-cell lymphoma 2; BTK=Bruton’s tyrosine kinase; BTKi=Bruton’s tyrosine kinase inhibitor; MM=multiple myeloma; MRD=measurable residual disease; PFS=progression-free survival.
References: 1. Xu J, Dong X, Huang DCS, Xu P, Zhao Q, Chen B. Current advances and future strategies for BCL-2 inhibitors: potent weapons against cancers. Cancers (Basel). 2023;15(20):4957. 2. Valentin R, Grabow S, Davids MS. The rise of apoptosis: targeting apoptosis in hematologic malignancies. Blood. 2018;132(12):1248-1264. 3. VENCLYXTO. European Union Summary of Product Characteristics. AbbVie Deutschland GmbH & Co. KG; 2025. 4. Deng J, Isik E, Fernandes SM, Brown JR, Letai A, Davids MS. Bruton’s tyrosine kinase inhibition increases BCL-2 dependence and enhances sensitivity to venetoclax in chronic lymphocytic leukemia. Leukemia. 2017;31(10):2075-2084. 5. Tam CS, Anderson MA, Pott C, et al. Ibrutinib plus venetoclax for the treatment of mantle-cell lymphoma. N Engl J Med. 2018;378(13):1211-1223. 6. Yue X, Chen Q, He J. Combination strategies to overcome resistance to the BCL2 inhibitor venetoclax in hematologic malignancies. Cancer Cell Int. 2020;20(1):524. 7. Wierda WG, Brown J, Abramson JS, et al. NCCN Guidelines® insights: chronic lymphocytic leukemia/small lymphocytic lymphoma, version 2.2026. J Natl Compr Canc Netw. 2026;24(3):68-80. 8. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma V.2.2026. © National Comprehensive Cancer Network, Inc. 2025. All rights reserved. Accessed December 22, 2025. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way. 9. Wallin M, Ko S, Shah P, Boisclair S, Gladstone D, Rampersaud T. Real-world outcome of low-frequency outpatient monitoring for venetoclax initiation in CLL: single-center experience. Blood. 2025;146(suppl 1):7919. 10. Jacobs R, Fletcher L, Rettew A, et al. Best practices to overcoming challenges in initiating venetoclax for patients with chronic lymphocytic leukemia: results from a United States community-based healthcare practitioner survey. Blood. 2024;144 (suppl 1):2268-2269. 11. Goldstein J, Kim WS, Yoon SE, et al. Optimizing circulating tumor DNA limits of detection for DLBCL during first line therapy. Blood. 2023;142(suppl 1):187-189. 12. Szalat RE, Anderson KC, Munshi NC. Role of minimal residual disease assessment in multiple myeloma. Haematologica. 2024;109(7):2049-2059. 13. Fenske TS, Wang XV, Till BG, et al. Lack of benefit of autologous hematopoietic cell transplantation (auto-HCT) in mantle cell lymphoma (MCL) patients (pts) in first complete remission (CR) with undetectable minimal residual disease (uMRD): initial report from the ECOG-ACRIN EA4151 phase 3 randomized trial. Blood. 2024;144(suppl 2):LBA-6-LBA-8. 14. Pratz KW, Jonas BA, Pullarkat V, et al. Measurable residual disease response and prognosis in treatment-naïve acute myeloid leukemia with venetoclax and azacitidine. J Clin Oncol. 2022;40(8):855-865. 15. Bernardi M, Ferrara F, Carrabba MG, et al. MRD in venetoclax-based treatment for AML: does it really matter? Front Oncol. 2022;12:890871. 16. Davids MS, Lampson BL, Tyekucheva S, et al. Acalabrutinib, venetoclax, and obinutuzumab as frontline treatment for chronic lymphocytic leukaemia: a single-arm, open-label, phase 2 study. Lancet Oncol. 2021;22(10):1391-1402. 17. Al-Sawaf O, Robrecht S, Zhang C, et al. Venetoclax-obinutuzumab for previously untreated chronic lymphocytic leukemia: 6-year results of the randomized phase 3 CLL14 study. Blood. 2024;144(18):1924-1935. 18. Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328-e346. 19. Kumar SK, Harrison SJ, Cavo M, et al. Venetoclax or placebo in combination with bortezomib and dexamethasone in patients with relapsed or refractory multiple myeloma (BELLINI): a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2020;21(12):1630-1642. 20. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Multiple Myeloma V.5.2026. © National Comprehensive Cancer Network, Inc. 2026. All rights reserved. Accessed January 9, 2026. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
This is a global website and is intended for healthcare professionals. The information on this site is intended for educational purposes only and is not country-specific.